If you run a medical practice, HIPAA compliance is not a project you finish once and file away. It is an ongoing responsibility that touches your front desk, your servers, your vendors, and every staff member who can see a patient record. The rules have not changed overnight, but the environment around them has. Cyberattacks on healthcare have grown sharper, federal penalty amounts were adjusted upward in early 2026, and a major update to the HIPAA Security Rule is working its way through the rulemaking process. A practical HIPAA compliance checklist gives you a way to see your obligations clearly, find the gaps before a regulator or an attacker does, and prove that your practice took its duties seriously. This guide walks through what HIPAA actually requires of a medical practice in 2026, the full checklist organized the way the law itself is organized, the mistakes that most often trigger enforcement, and how to keep the whole thing maintained rather than letting it drift.
The Ultimate HIPAA Compliance Checklist for Medical Practices in 2026

What HIPAA Compliance Actually Means for a Medical Practice
The Health Insurance Portability and Accountability Act sets national standards for protecting patient health information. Most medical practices are what HIPAA calls a covered entity, meaning a healthcare provider that transmits health information electronically in connection with a transaction such as a claim or an eligibility check. If that describes your practice, HIPAA applies to you regardless of your size. A solo physician with one part-time biller carries the same core obligations as a multi-location group.
The information HIPAA protects is called protected health information, or PHI. In plain terms, PHI is any information that identifies a patient and relates to their health, their care, or payment for that care. When that information exists in electronic form, it is called ePHI, and it carries additional technical requirements. A patient's name on its own is not PHI. That same name attached to an appointment, a diagnosis, an insurance ID, or a billing record is.
HIPAA itself is built from a few connected rules, and a useful HIPAA compliance checklist follows their structure:
- The Privacy Rule governs how PHI may be used and disclosed, and gives patients rights over their own records, including the right to access them.
- The Security Rule governs ePHI specifically, requiring administrative, physical, and technical safeguards.
- The Breach Notification Rule defines what counts as a breach and who must be told, and when, after one occurs.
- The Enforcement Rule sets out how the Office for Civil Rights, or OCR, investigates complaints and imposes penalties.
Understanding this structure matters because compliance is not a single switch. A practice can have excellent technology and still fail the Privacy Rule by mishandling a records request, or have strong policies on paper and still fail the Security Rule by never completing a risk analysis.

Why a HIPAA Compliance Checklist Matters More in 2026
Two forces make this a particularly important year to take a structured approach rather than relying on memory or habit.

The Real Cost of Getting It Wrong
HIPAA civil penalties are organized into four tiers based on how culpable the practice was, ranging from violations the practice genuinely did not know about to willful neglect that was never corrected. The dollar amounts are adjusted for inflation each year. The most recent adjustment took effect on January 28, 2026, and it raised the figures across all tiers. For the most serious tier, the maximum annual penalty now exceeds two million dollars per category of violation. A single breach can trigger penalties in more than one category at the same time.
Two points are easy to miss and worth stating plainly. First, OCR enforces HIPAA against practices of every size, and small practices are investigated regularly, often because they lack dedicated compliance staff and layered cybersecurity solutions. Second, federal penalties are not the only exposure. In California, the Confidentiality of Medical Information Act adds a separate layer. Unlike HIPAA, CMIA gives patients a private right of action, meaning an individual patient can sue a practice directly for mishandling their medical information, with statutory damages on top of actual damages. For a practice in the Los Angeles area, that state-level risk is a real and additional reason to keep compliance tight.
The Proposed 2026 HIPAA Security Rule Update
This is the part of the conversation where accuracy matters most, because it is widely misreported. OCR published a Notice of Proposed Rulemaking on the HIPAA Security Rule in the Federal Register on January 6, 2025. It would be the first major overhaul of the Security Rule in over two decades. As of May 2026, that update is still a proposed rule. It has not been finalized, and it is not yet law. OCR's regulatory agenda has listed a mid-2026 target for a final rule, but the agency has not confirmed that timeline, and many industry groups have asked for changes, so a delay is entirely possible.
If the rule is finalized broadly as proposed, the headline change is that several safeguards that are currently flexible would become firm requirements. The proposal would, among other things:
- Require encryption of ePHI both at rest and in transit, removing the current flexibility that lets practices treat encryption as optional if they document a reason.
- Require multi-factor authentication for systems that access ePHI.
- Set fixed intervals for technical testing, including regular penetration testing and more frequent vulnerability scanning.
- Require written technology asset inventories and network maps.
- Expand incident response and reporting obligations and tighten oversight of business associates.
When a final rule does publish, covered entities are expected to get a compliance window of roughly 240 days. The practical takeaway for 2026 is this: do not treat the proposal as a current legal requirement, but do treat it as a strong signal of where the standard is heading. A practice that is already encrypting ePHI, enforcing multi-factor authentication, and testing its systems will face an easy transition. A practice that waits for the final rule will be scrambling.
The Ultimate HIPAA Compliance Checklist for Medical Practices in 2026
The checklist below follows the structure of the HIPAA rules themselves. Work through it section by section. For each item, the goal is not just to do the thing, but to be able to show documentation that you did it. In a HIPAA investigation, undocumented compliance is treated much like no compliance at all.

Administrative Safeguards
These are the policies, assignments, and processes that govern how your practice manages security day to day. They are the most common point of failure in enforcement cases, and several of them, such as the contingency plan, depend on dependable data backup and disaster recovery being in place.
- Conduct a thorough, practice-wide security risk analysis that identifies where ePHI lives, how it moves, and what threats it faces. This is the single most important item, and the most frequently missing one.
- Maintain a documented risk management process that shows how identified risks are being reduced over time.
- Designate a HIPAA Security Officer and a HIPAA Privacy Officer. In a small practice this may be the same person, but the role must be formally assigned.
- Train every workforce member on HIPAA basics and on your specific policies, and document who was trained and when.
- Maintain a written sanction policy that defines consequences for staff who violate HIPAA rules, and apply it consistently.
- Regularly review information system activity, including access logs and audit reports, to spot unusual behavior.
- Implement access management procedures that grant each staff member only the minimum access their job requires.
- Maintain a contingency plan covering data backup, disaster recovery, and emergency operations so that patient care and records survive a system failure or attack.
- Perform a periodic evaluation to confirm your safeguards still match your environment after changes in staff, software, or workflow.
Physical Safeguards
These protect the physical spaces and devices where ePHI is stored or accessed.
- Control physical access to areas with servers, network equipment, and records, using locks, badges, or other appropriate measures.
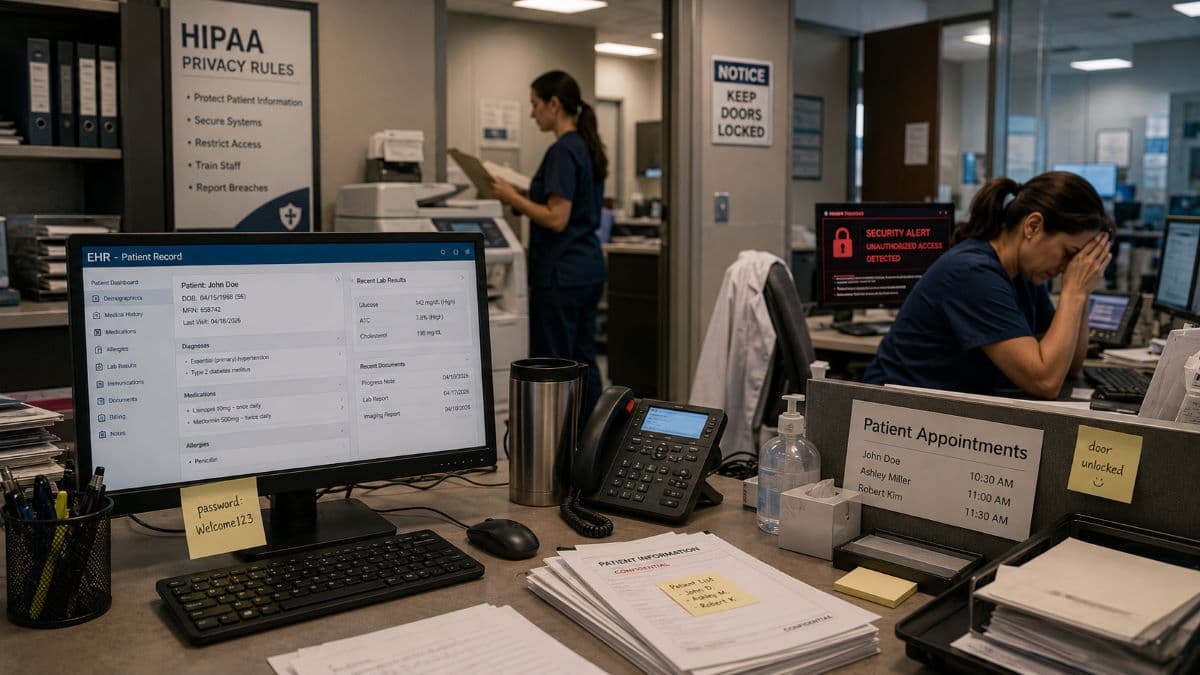
- Position and secure workstations so that screens displaying PHI are not visible to patients or visitors in waiting and reception areas.
- Maintain device and media controls that govern how laptops, phones, drives, and backup media are tracked, reused, and disposed of.
- Securely wipe or destroy any device or media before disposal, so that no recoverable ePHI leaves your control.
Technical Safeguards
These are the technology controls that protect ePHI inside your systems.
- Assign a unique user ID to every individual so that all activity can be traced to a specific person, and never use shared logins.
- Enable automatic logoff on workstations so that an unattended screen does not expose patient records.
- Encrypt ePHI at rest and in transit. This is currently flexible under the existing rule, but it is strongly recommended now and is likely to become mandatory under the proposed update.
- Maintain audit controls that log access to systems containing ePHI, and actually review those logs.
- Implement integrity controls that protect ePHI from improper alteration or destruction.
- Use strong authentication, and enforce multi-factor authentication for remote access and for systems that hold ePHI.
- Secure all transmission of ePHI, including email, patient portals, and connections to outside labs or specialists.
Organizational Requirements and Business Associate Agreements
Your compliance does not stop at your own walls. Any outside vendor that creates, receives, maintains, or transmits PHI on your behalf is a business associate, and they extend your risk. This is especially true of the cloud platforms that hold email and patient files, which is why correctly configured managed Microsoft 365 services matter for practices that run on them.
- Identify every business associate, including your EHR vendor, billing company, IT provider, cloud and email host, shredding service, and answering service.
- Have a signed Business Associate Agreement in place with each one before any PHI is shared. A missing BAA is a frequent and avoidable violation.
- Confirm that major platform vendors will sign a BAA for the specific service you use. For example, a practice running on cloud productivity tools should ensure the appropriate agreement covers email and file storage.
- Maintain written policies and procedures for all of the safeguards above, and keep them current.
- Provide patients with a Notice of Privacy Practices, and review it for required updates. Practices that handle substance use disorder treatment information should note that revised Part 2 rules carried a February 2026 compliance date for related notice updates.
- Retain HIPAA documentation for at least six years from the date it was created or last in effect.

Breach Notification and Incident Readiness
Even a well-run practice can experience a breach. What separates a manageable incident from a damaging one is preparation.
- Maintain a written incident response plan that defines who does what when a possible breach is discovered.
- Establish a process for assessing whether an incident rises to the level of a reportable breach.
- Notify affected patients without unreasonable delay and within 60 days of discovering a breach.
- Notify HHS, within 60 days for breaches affecting 500 or more individuals, and through the annual submission process for smaller breaches.
- Notify prominent media outlets when a breach affects more than 500 residents of a state or jurisdiction.
- Document every incident and every notification, including incidents you concluded were not reportable.
Preparing Now for the Proposed Security Rule Changes
These items are not yet legally required, but completing them positions your practice well and improves your security regardless of what the final rule says. Where the proposal calls for fixed testing intervals, scheduled penetration testing is a sensible way to stay ahead of it.
- Move toward encrypting all ePHI at rest and in transit if you have not already.
- Enforce multi-factor authentication everywhere ePHI can be reached.
- Create and maintain a written inventory of technology assets and a map of your network.
- Schedule regular penetration testing and vulnerability scanning rather than treating security testing as a one-time event.
- Review and strengthen the security expectations written into your business associate agreements.
Common HIPAA Compliance Mistakes Medical Practices Make
Most enforcement actions do not involve exotic failures. They involve the same handful of gaps repeated across thousands of practices. Recognizing them is the fastest way to reduce your exposure.
The most common mistake is treating the risk analysis as optional or as a formality. OCR has cited the absence of a genuine, practice-wide risk analysis in case after case, including the investigation behind the largest HIPAA settlement on record, which involved a health insurer and a breach affecting tens of millions of people. A risk analysis is the foundation of the Security Rule, and a checklist cannot substitute for it.
A second frequent mistake is assuming that buying a product makes you compliant. Vendors often market software as HIPAA compliant, which can be misleading. Software can support your compliance, but compliance is something your practice does, through policies, training, documentation, and oversight. No single purchase delivers it.
Other recurring gaps include missing business associate agreements, no documented or current workforce training, failing to provide patients access to their own records within the required timeframe, shared logins that make activity untraceable, and a Notice of Privacy Practices that has not been updated in years. None of these are expensive to fix, and structured compliance and risk management services exist precisely to keep them from being overlooked. All of them are expensive to ignore.
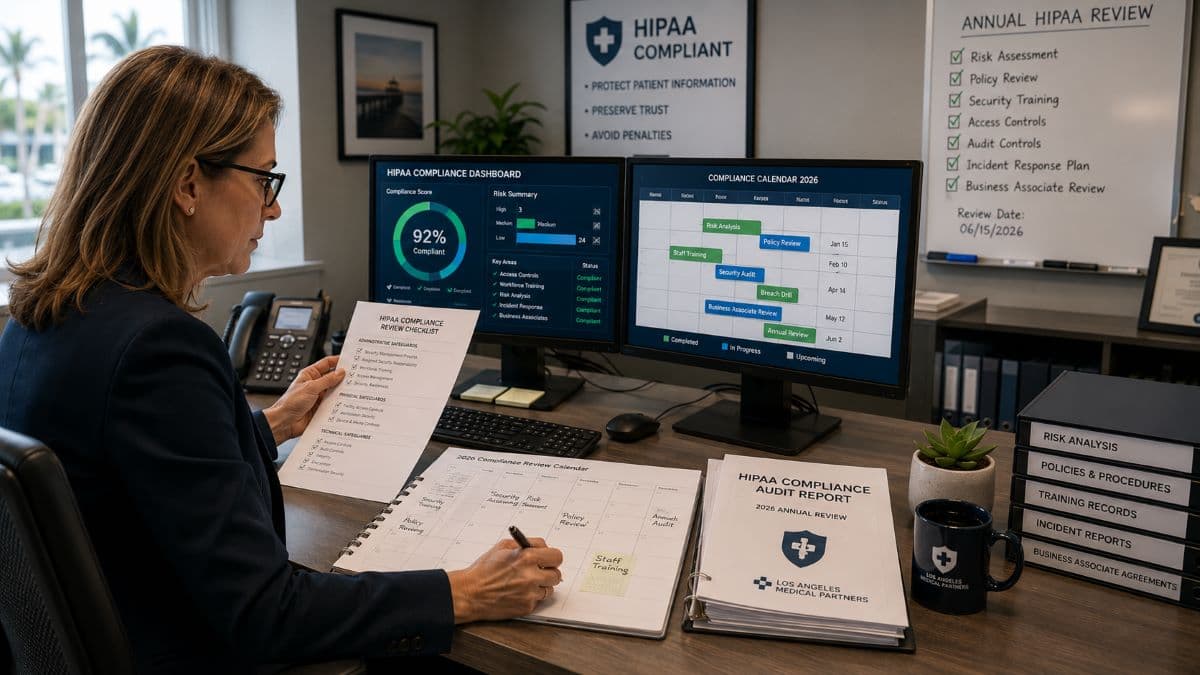
How Often Should You Review Your HIPAA Compliance Checklist?
HIPAA compliance is continuous, not annual. The risk analysis and your written policies should be formally reviewed at least once a year, and also whenever something material changes, such as a new EHR, a move to a new office, a new line of service, or significant staff turnover. Workforce training should be refreshed annually and delivered to new hires as part of onboarding. Access logs and audit reports should be reviewed on a routine schedule, not just after an incident. Business associate agreements should be checked whenever you add or change a vendor. Ongoing managed IT services can carry much of this routine load, and treating the HIPAA compliance checklist as a living document, rather than a once-a-year obligation, is what keeps small gaps from quietly becoming reportable breaches.
When to Bring in Outside Help
Many medical practices reach a point where the compliance and security workload outgrows what office staff can reasonably manage alongside patient care. That is a normal stage, not a failure. The technical safeguards in particular, encryption, audit logging, access control, secure backups, and the testing the proposed rule would require, sit at the intersection of healthcare regulation and information technology, and they benefit from specialist attention.
This is where structured support is worth considering. The right partner keeps the risk analysis, documentation, and policy work current, hardens the technical safeguards, and provides the monitoring and maintenance that make compliance sustainable instead of a yearly fire drill.
GlobeVM is a managed IT and cybersecurity firm serving small and mid-sized businesses across the Los Angeles area, with CCSP-certified expertise and a practical focus on HIPAA compliance. That local presence matters for healthcare practices, because California's CMIA adds state-level exposure that a national vendor may overlook.
Frequently Asked Questions
If you want a clear picture of where your practice stands today, a HIPAA-focused risk assessment from a qualified local partner is the most direct way to find your gaps before a regulator or an attacker does.
Comments
0 Comments